Loading...
New federal cuts to Canada's refugee health program take effect this week. The people who work with asylum seekers say the consequences could be devastating.
Natasha Shepherd
Writer

April 29, 2026 The LocaL by Wency Leung with photography by Chloë Ellingson
New federal cuts to Canada's refugee health program take effect this week. The people who work with asylum seekers say the consequences could be devastating.
Diana Gallego, the co-executive director of Toronto’s FCJ Refugee Centre, worries about the changes that the federal government is making to its Interim Federal Health Program. She’s worried it will mean refugees and asylum seekers won’t get the medicine or dental work or eye exams they need. And in particular, she’s worried those requiring mental health counselling won’t be able to get it.
Every Monday, known as “intake day” at her centre, newcomers pack into the waiting room of the converted brick house, near Dufferin Street and St. Clair Avenue West. They come looking for advice on how to apply for legal aid or how to find transitional housing, to sign up for English classes, to visit the primary health clinic, or access the other programs and services the centre provides.
Among those who rely on the centre, Gallego said, are refugees and asylum seekers who have endured war, persecution, sexual violence, and torture before seeking protection in Canada. Having to restart their lives here, often without family support, can also take an enormous mental and emotional toll. Access to a psychologist or psychotherapist can be critical to their integration, not only because it supports their well-being but because their claims for protection may be jeopardized if they have unaddressed trauma, Gallego said. Untreated post-traumatic stress disorder, for example, could hamper their ability to answer an Immigration and Refugee Board adjudicator’s questions, and without records of having seen a mental health professional, they may not be believed, she said.
“The adjudicator can say, ‘I don’t see that you went to see a clinician. I don’t see that you went to see a psychologist…Where is there clinical evidence?’” Gallego said.
Psychological counselling and psychotherapy are fully covered by the Interim Federal Health Program (IFHP), but not for much longer.
The IFHP, created in 1957, is meant to provide stopgap coverage to refugees and asylum seekers until they qualify for provincial insurance, like OHIP, and extended health benefits, like those available through social assistance programs.
Starting May 1, however, it will require beneficiaries to directly pay for a portion of what the
government calls supplemental health costs. Basic health services, like doctors’ visits and care provided in hospitals, will still be provided without charge. But refugees and asylum seekers will be required to shell out for 30 percent of health products and services, such as dental care, vision care, counselling, and medical equipment like wheelchairs, prosthetics, and diabetic supplies. There will be new limits to the amount of care the program covers, like the number of psychotherapy or counselling sessions and the maximum cost of dental restorations. And beneficiaries will also be required to pay $4 for each prescription medication. Depending on their needs, a patient’s co-payments in a given year could easily add up to hundreds of dollars.
It’s the co-payment requirement for counselling that Gallego finds most troubling. “One of the most outrageous cuts is that now you have to pay extra money to have to talk to somebody that can listen,” she said.
Atwia, an asylum seeker from Uganda, isn’t sure she’ll be able to afford the new co-payments. Atwia,
who is using a pseudonym to discuss her health issues and status, suffers from anxiety. She currently relies on the IFHP to cover her daily medications and regular therapy sessions.
She came to Canada on her own in March of 2025 to seek safety, she said. Her transition to Toronto “has not been easy.”
“Day in, day out. You’re crying, you know, in worry, in fear,” she said. Combined with the trauma that led her to seek protection here, that’s resulted in anxiety and depression.
The treatment she is receiving is “a process,” she said. Her doctor has been adjusting her prescriptions to find the appropriate dose. When her condition worsened, she increased the frequency of her therapy sessions. Because her mental health care has so far been provided without charge, Atwia does not know how much she will be expected to co-pay, though she anticipates it will be costly.
That worries her, she said, since she knows she needs this care, and she is still struggling to find a job.
“Seriously, it’s not been easy,” she said again, but added she’s trying to remain positive. “I have to appreciate that Canada gives me a chance to live freely.”
Even without the new co-payment requirements, accessing health care through the IFHP can be extremely difficult. Time and again, palliative care doctor Humaira Saeed has seen patients fall through the cracks.
Asylum seekers are entitled to IFHP coverage for basic and supplemental health care for the duration of their refugee determination process, while resettled refugees can receive supplemental IFHP coverage for up to 12 months.
But often they aren’t able to access the same kinds of care, like wound care or support at home, that OHIP patients receive, Saeed said. And for patients with life-limiting illnesses like cancer, heart failure, or liver failure, that often means they disproportionately suffer from pain and other symptoms, and wind up in hospital, where they tend to stay for longer periods.
Navigating the health care system can be challenging for newcomers in the first place, but the IFHP presents its own set of hurdles. Even though the program is funded by the federal government, the private insurance company Medavie Blue Cross is contracted to run it. Saeed likens the IFHP to workplace extended health benefits; it’s a “parallel system” to the OHIP system, she said. Health providers must register with Medavie Blue Cross to work with IFHP patients, and they need to obtain the insurance company’s approval, and certain pre-approvals, to cover patient expenses.
The paperwork can be onerous and the payment system isn’t sustainable for certain business models. As a result, there are relatively few IFHP providers, Saeed said.
In 2024, she co-founded a non-profit called GPS Health Navigators, serving refugees on IFHP in the Greater Toronto Area and Hamilton. It helps patients, especially those requiring palliative care, get past these barriers and connect them with providers, services, medications, and equipment. But in light of the May 1 changes, Saeed has already heard from several pharmacies and medical equipment companies saying they will no longer be able to support patients who can’t afford the 30 percent co-payments. They’re barely breaking even as it is, they’ve told her. They fear they won’t be able to recuperate their costs under the new co-payment model.
In an email to The Local, Immigration, Refugees and Citizenship Canada (IRCC) said the changes to the IFHP are necessary, and that early estimates indicate they could result in about $126.6 million in savings in 2026-27, and $231 million after that.
“Introducing co-payments for supplemental health products and services will help manage growing demand, keeping the IFHP sustainable over the long term,” it said. It added that the changes would align the program “more closely with many other health benefit programs, where Canadians often share part of the cost of their supplemental health benefits.”
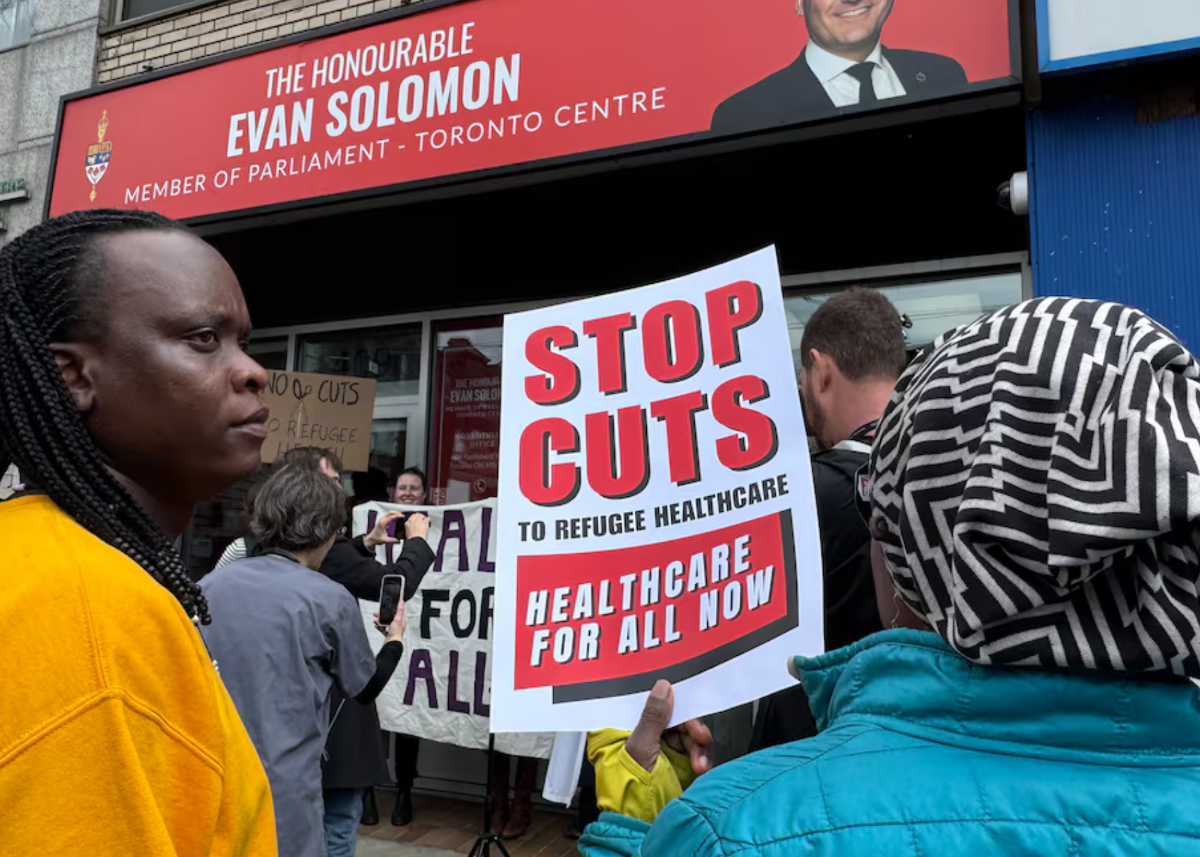
Those who provide care for refugees and asylum seekers disagree. Since the government announced the changes, health care professionals across the country, including from the Canadian Refugee Health Network, The No Cuts to Care Coalition, and the coalition of national health organizations HEAL, have been speaking at rallies, writing letters to the Immigration Minister, and speaking to the media in protest.
For starters, seniors and people on social assistance receive similar health coverage without the same co-payment requirements, said Vanessa Redditt, a family physician who provides care to some of the city’s most vulnerable people at several clinics in Toronto. She works at the Crossroads Clinic at Women’s College Hospital among others, and has been filling in at the FCJ Refugee Centre clinic. (The FCJ Refugee Centre clinic is meant for patients without OHIP or IFHP coverage. But some of the clinic’s patients later end up accessing IFHP, while others find their way to the clinic after losing their IFHP coverage.)
Moreover, the changes won’t actually result in savings, Redditt said, explaining they will only increase the costs of dealing with preventable complications and more serious illnesses when patients put off seeking care.
Redditt offered a hypothetical scenario: A patient with diabetes and hypertension may need multiple medications, requiring several $4 co-payments at once. If they forgo filling their prescriptions because they don’t have the money to pay for them, they could wind up in hospital and then a rehabilitation facility—“the most expensive parts of our health care system,” she said. If they suffer prolonged neurological effects and can’t return to the workforce, they may require disability benefits.
Redditt, Saeed, and other critics point to multiple research studies that support their economic, medical, and health policy rationales for opposing the introduction of co-payments. But their argument is also a moral one.
Paul Caulford, the clinic physician and executive director at The Canadian Centre for Refugee and Immigrant Healthcare in Scarborough, called the changes to the IFHP “discriminatory.”
“This is an inhumane approach,” he said—and one that comes amid hardening public sentiment toward newcomers. As the Liberal government has clamped down on immigration over the past year, tightening its borders and increasing its scrutiny of visa applications, the number of asylum seekers declined by 34 percent between 2024 and 2025, according to the IRCC.
But refugees are not immigrants, Caulford said: “They’re a humanitarian aspect to Canada’s identity.”
It wasn’t so long ago when Canadians showed overwhelming support for refugees during the Syrian refugee crisis in 2015, and again in the aftermath Russia’s 2022 invasion of Ukraine. Redditt said she still wells up when she thinks of the indelible image of two-year-old Alan Kurdi’s lifeless body washed ashore, having drowned while trying to cross the Mediterranean Sea to Europe with his Syrian family in 2015.
Even if she and her colleagues are unsuccessful in persuading the government to reverse its changes by May 1, Redditt said they don’t intend to give up their fight. After all, they’ve been down this road before. In 2012, the Conservative government made deep cuts to the IFHP, prompting refugee advocates—many of the same ones protesting the changes today—to take their case to the Federal Court. That court determined the cuts were “cruel and unusual” in a 2014 ruling, and the health services were eventually reinstated.
Redditt admitted it may sound corny, but the work and advocacy that often keeps her toiling late into the night is driven by a firmly held conviction. “If we live in a society that tolerates injustice, if we live in a society that harms the most vulnerable and erodes their rights…” she paused and gently shook her head. “What values do we have left?”
----------
Writer