Loading...
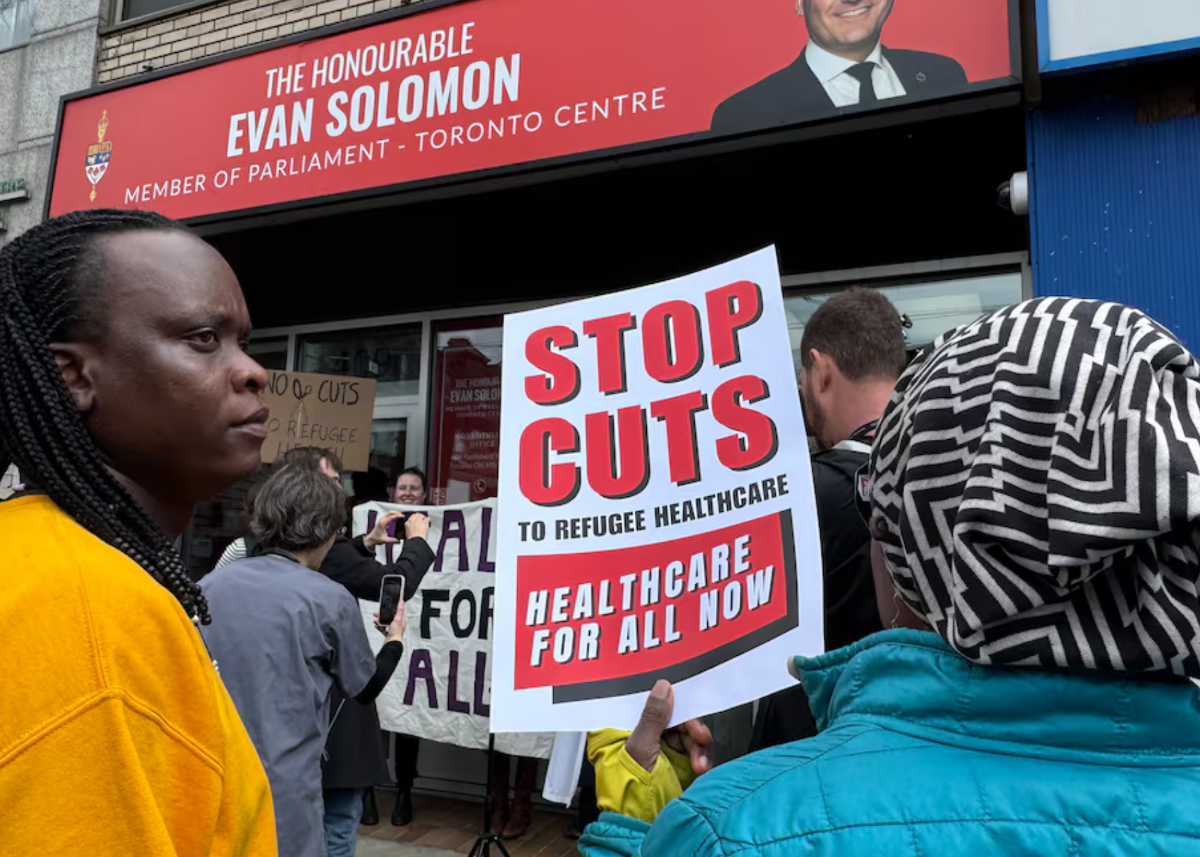
The Interim Federal Health Program, which provides health-care coverage to refugees and refugee claimants, has become the latest target in Canada’s increasingly polarized immigration debate. In February, Conservative Members of Parliament introduced a motion calling for significant cuts to the program, reviving memories of the unconstitutional reductions imposed by the Harper government in 2012.
Elizabeth Nola
Writer

BY Y.Y. BRANDON CHEN, The Hill Times, June 17, 2026
In practice, access to care under the IFHP is often far more limited than critics suggest.
The Interim Federal Health Program, which provides health-care coverage to refugees and refugee claimants, has become the latest target in Canada’s increasingly polarized immigration debate. In February, Conservative Members of Parliament introduced a motion calling for significant cuts to the program, reviving memories of the unconstitutional reductions imposed by the Harper government in 2012.
Although the motion was defeated, calls to scale back the Interim Federal Health Program (IFHP) have persisted. These arguments often rely on misinformation and fearmongering rather than evidence, portraying refugee claimants as opportunists exploiting public benefits.
One of the most common allegations against the IFHP is that it provides refugees and refugee claimants with greater health coverage than that available to Canadians. In reality, IFHP benefits are comparable to those available to low-income individuals through provincial and territorial social assistance programs. This design reflects the reality that many refugees and refugee claimants arrive in Canada after fleeing war, persecution, or other serious human rights violations, often with few financial resources as they establish their lives in a new country.
As such, IFHP benefits are far from the “luxury” or “all-inclusive” coverage that critics often portray. Dental care provides a useful example. The IFHP’s dental coverage is largely restricted to treatment required for the emergency relief of pain or infection, and many procedures require prior authorization before reimbursement will be approved. Routine services like dental cleanings and orthodontic treatment are not covered.
Even obtaining services that are covered can be difficult. Research has shown that IFHP beneficiaries face significant barriers in accessing care. Health-care providers are under no obligation to register with the program, and many choose not to do so.
Even when refugees and refugee claimants seek care from participating providers, they may be denied services or asked to pay privately because of confusion about the IFHP’s coverage rules. In practice, access to care under the IFHP is often far more limited than critics suggest.
Recent changes requiring refugees and refugee claimants to make copayments for prescription drugs, dental care, and other supplemental benefits are widely expected to create further access barriers.
Another recurring criticism of the IFHP is that it encourages so-called “bogus refugees” to come to Canada. The Federal Court considered this argument in 2014 when reviewing the Harper government’s cuts to the program and found it to rest on subjective perceptions rather than empirical evidence. Immigration officials were unable to present any evidence that Canada’s refugee process was systematically exploited by those simply seeking to access publicly funded health care.
The IFHP does not provide health coverage to anyone who merely files a refugee claim. Individuals found ineligible to claim refugee protection in Canada, as well as those who withdraw or are deemed to have abandoned their claims, are not entitled to IFHP coverage.
Critics also note that IFHP coverage for unsuccessful refugee claimants ends only when a removal order is enforced, implying that public health care is being extended to people with fraudulent claims. This framing overlooks two important facts.
First, many individuals facing removal are engaged in ongoing legal proceedings and may lawfully remain in Canada while those processes unfold. Second, refugee determinations are not infallible: studies suggest that more than one-third of initially rejected claimants ultimately succeed on appeal, while others obtain permanent resident status through alternative immigration processes.
The IFHP’s coverage rules reflect these realities rather than assuming that every unsuccessful claimant is simply abusing the system.
In fact, research has consistently shown that people at risk of deportation frequently avoid seeking health care due to fear of attracting attention from authorities. They are unlikely a significant driver of IFHP expenditures. To suggest otherwise is unsupported by evidence, and serves primarily to stoke resentment against an already vulnerable group.
Current attacks on the IFHP draw strength from a broadly shared frustration: essential services such as prescription drugs and dental care remain out of reach for too many people. But the answer to these gaps lies not in reducing coverage for refugees and refugee claimants. It lies in expanding access for everyone.
Instead of resorting to misinformation and us-versus-them rhetoric, policymakers should work toward expanding universal health care, including by building on recent federal dental care and pharmacare initiatives, so that all Canadians can access the care they need.
Writer
KLHIISA Writer